
Chara Oraipoulou , BSc, MRes. Biologist, Sr. Clinical Embryologist (ESHRE Certified)
, BSc, MRes. Biologist, Sr. Clinical Embryologist (ESHRE Certified)
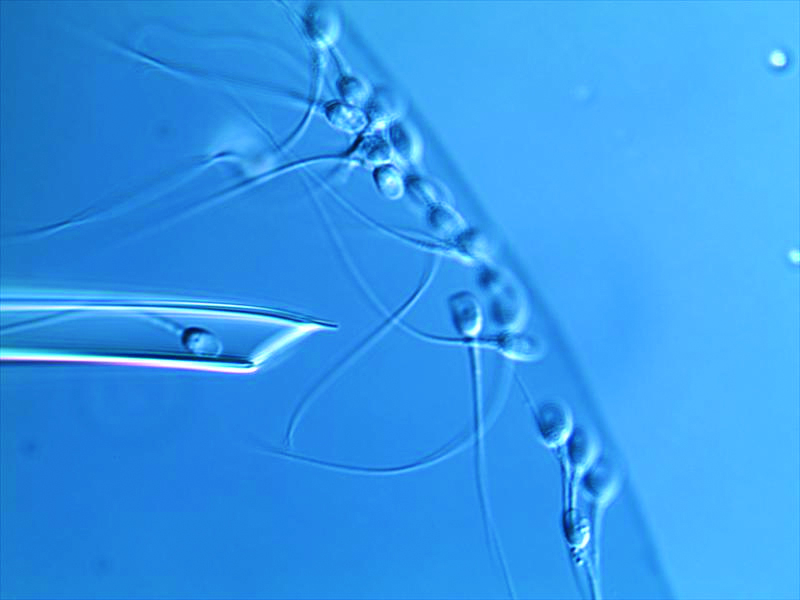
Non-obstructive azoospermia (NOA) is marked by absence of spermatozoa during ejaculation due to pathologic spermatogenesis. Nowadays, a significant percentage of men with NOA can have children, since the likelihood of locating spermatozoa following testicular biopsy is close to 50%. The question is whether the laboratory and clinical outcome differs depending on the quality of the testicular tissue from where the spermatozoa used for microfertilisation (ICSI) originate. The answer to this question was examined as part of an Embryolab study, also taking into account the effect of possible testicular tissue cryopreservation.
Testicular tissue quality following biopsy is determined by three key parameters: the spermatozoa concentration in the testicular sample, the presence of motile spermatozoa and the testicular spermatozoa morphology. Two groups were used to conduct the study: a) good-quality and b) low-quality testicular tissue samples. The aim was to investigate their effect on the fertilisation rate, the embryonic development up to day three, the positive beta-HCG rate and the birth rate. In addition, the effect of testicular tissue cryopreservation was assessed against the above rates.
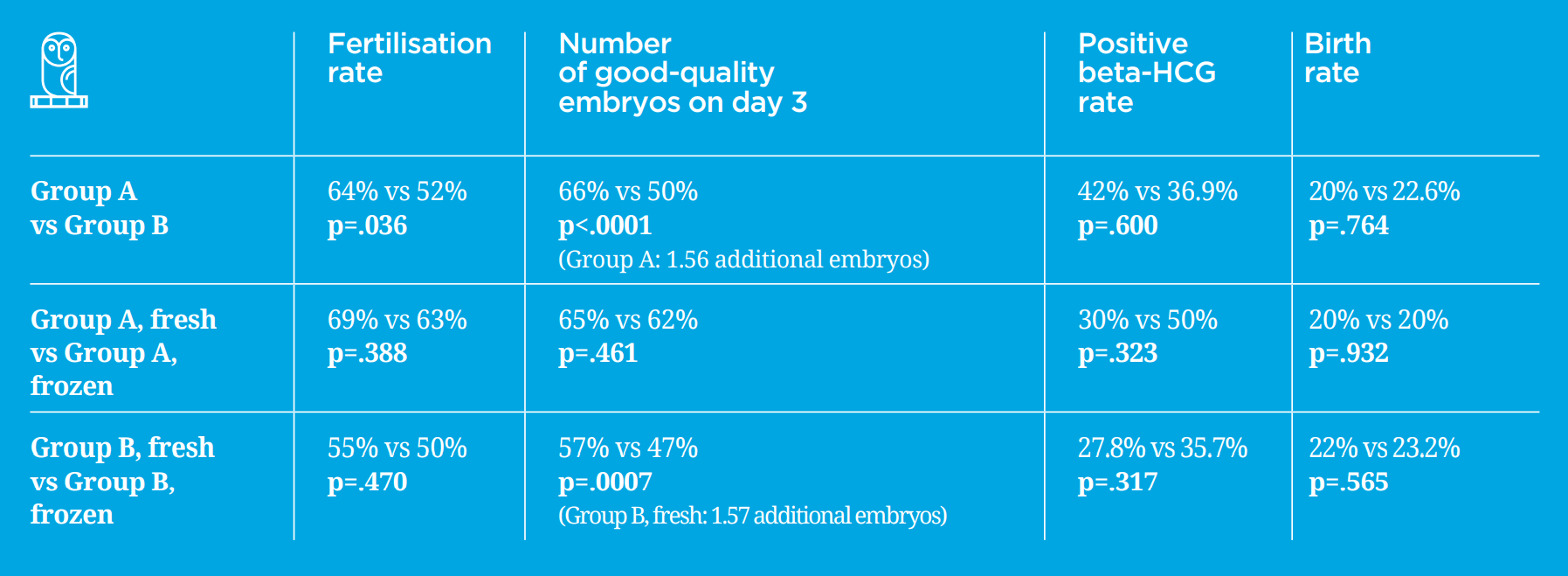
According to the Unit’s published findings (https://doi.org/10.1111/and.14040), the quality of testicular tissue does not affect the pregnancy and birth rates (Table 1). However, it is interesting that the low-quality testicular samples are associated with lower fertility rates and produce fewer good-quality embryos on day three. Consequently, investing time to find suitable testicular spermatozoa for fertilisation is of essence even in low-quality testicular samples. Despite all this, the experience of the operator in determining the time frame for searching for spermatozoa plays an important part, since it has been proven that when the search time exceeds a certain limit, the fertilisation and pregnancy rates drop in cycles with fresh eggs.
The cryopreservation of testicular tissue does seem to influence the clinical outcome, since there is no statistically significant difference in the pregnancy and birth rates among fresh and frozen testicular spermatozoa (Table 1). Nevertheless, low-quality fresh testicular samples seem to lead to better outcomes in terms of day three embryo formation, compared to frozen testicular samples of similar quality.
To date, the possibility of predicting the ability of testicular spermatozoa to support embryonic development is limited. These data, coupled with additional studies, could assist in creating a model for predicting the reproductive potential of testicular spermatozoa, so as to improve the treatment of men with non-obstructive azoospermia.
Table 1
Statistical results from the comparison of the two groups of testicular samples (Group A: good-quality testicular samples, Group B: low-quality testicular samples) to determine their effect on the fertility rate, the number of good-quality day 3 embryos, the positive beta-HCG rate and the birth rate.


{kind=link}
{kind=link}
{kind=link}